Mouthguards for the prevention of oro-facial trauma in sport
The Faculty of Sport & Exercise Medicine UK invited a panel to convene and issue a position statement on the use of mouthguards in sport. Contributors included Sport & Exercise Medicine, Sports Dentistry, Sports Science, athlete and coach perspectives to provide up-to-date guidance on the use of mouthguards in sport for the prevention of orofacial trauma (OFT). This position statement is aimed at health professionals, sports participants, educators, coaches, and parents/carers.
A well-fitting mouthguard should be used by all athletes if there is an anticipated risk of OFT, including dental injury, during competition and training. Mouthguard use is associated with both a reduction in the risk of sustaining an orofacial injury1,2 and a reduction in the severity of dental injuries in athletes.3 Clear recommendations on mouthguard use by coaches, parents and sports governing bodies, on how to fit and maintain mouthguards, can help to promote athlete welfare and is key for primary injury prevention.4 We recommend that governing bodies, health professionals in sport, and key sports stakeholders integrate this statement into their medical guidance together with an implementation strategy.
The burden of orofacial trauma in sport
Sport-related OFT can have a long-term impact on athletes’ ability to train, breathe effectively, and cosmetic appearance.4 In some instances, athletes may need ongoing maintenance of restorative dental treatment after sustaining OFT. This is a particular concern for adolescent and younger athletes with developing dentition and has the potential for a lifelong treatment burden on oral health and wellbeing in this group.
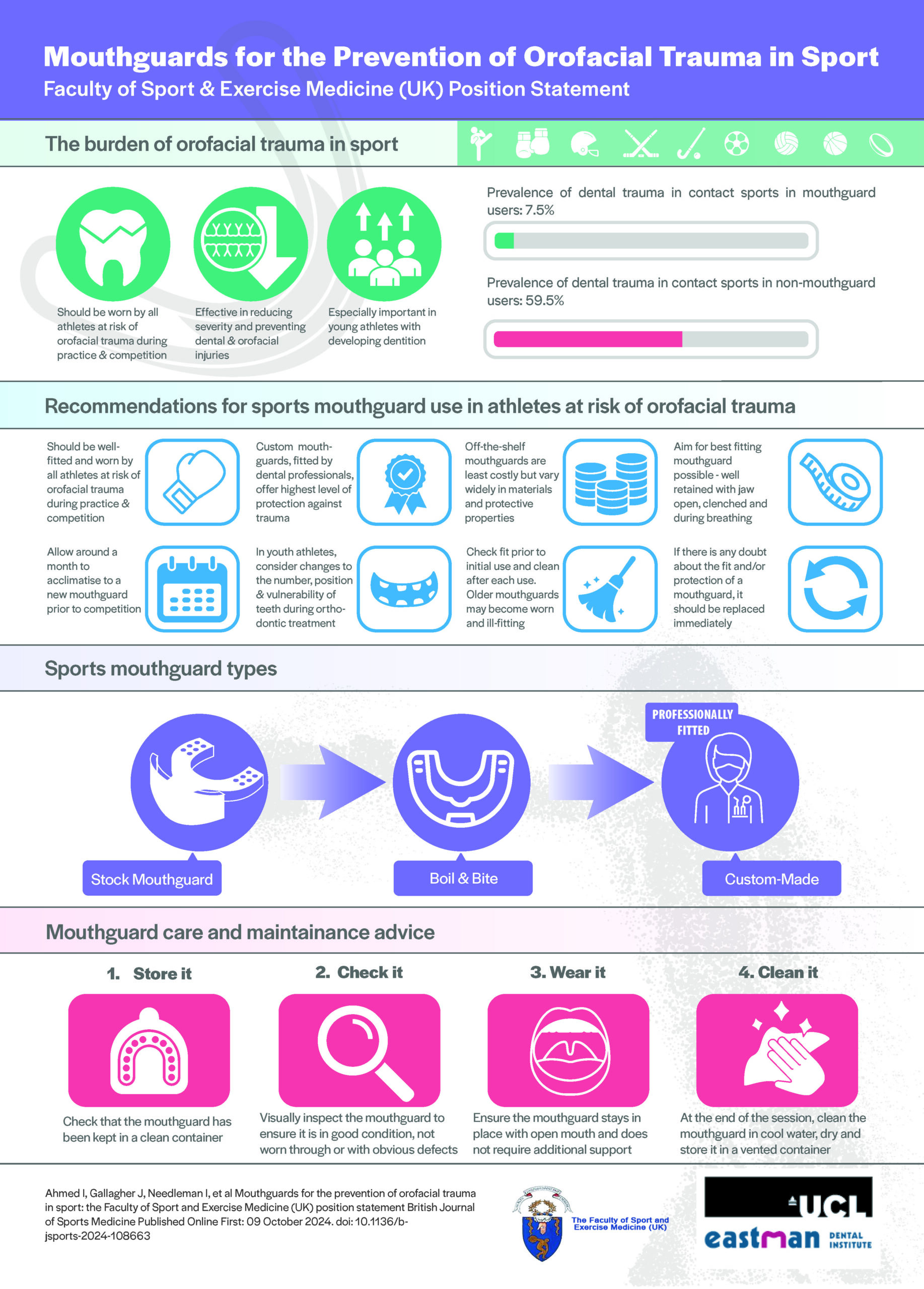
The incidence of OFT varies by individual sports. However, studies have shown that athletes at both the grassroots and elite levels, competing in “at risk” combat, collision, and contact sports are most affected.5 (Table 1) The prevalence of dental trauma is higher in non-mouthguard users (59.5%) than in mouthguard users (7.5%) (contact sports).6 Meta-analysis has also shown that non-mouthguard use increased the risk of OFT (relative risk, 2.33) compared to mouthguard users in different sports.1 In the highest risk contact sports there remains a lack of awareness on how routine mouthguard use can prevent traumatic injuries to teeth7 .
Recommendations for sports mouthguard use in athletes at risk of orofacial trauma
1 – All athletes at risk of dental trauma or orofacial injury should wear a mouthguard that fits well throughout training and competition sessions.
2 – Custom mouthguards, fitted by a dental professional, offer the highest level of protection against dental trauma.
3 – Off-the-shelf mouthguards are the least costly and most widely available option globally but can vary in size, materials and protective properties.
4 – Athletes should aim to wear the best-fitting mouthguards possible, and at a minimum the mouthguard should be well-retained in both clenched jaws, breathing and in open mouth positions.
5 – When using a new mouthguard, allow a period of acclimatisation (~1 month of use prior to competition) so that athletes can get used to wearing the mouthguard and ensure comfort while breathing.
6 – Mouthguards designed for adolescent and youth athletes should consider changes in the position and number of teeth and potential orthodontic treatment during fabrication and fitting.
7 – The mouthguard fit should be checked before initial use and the mouthguard should be cleaned after each use. Older mouthguard may become worn, thin, and ill-fitting.
8 – If there is any doubt about the fit and/or protection of an existing mouthguard, it should be replaced immediately.
Implementing the use of sports mouthguards in at-risk athletes
Athletes commonly cite being required to wear a mouthguard by rule, advice from their coach, or being allowed a period to acclimatise to the mouthguard fit and material as positive influences on their adherence with mouthguard use. It is therefore important to factor these in when advocating for the use of a well-fitted dental mouthguard to prevent or at least minimise the severity of dental injuries sustained during sport.8 Awareness amongst athletes of the relative protective properties of different mouthguard types (i.e., custom made, boil & bite, stock) varies by level of sport, cost, and access to a dental professional. (Table 1)
A well-fitting, retentive mouthguard offers protection and significantly reduces the risk of injury to the dentition, soft tissues, the temporomandibular joint and intraoral bony structures.2,3,4,8 No negative impacts on performance have been demonstrated from well-fitting custom-made mouthguards.9,10 They are well-tolerated and do not impede communication between athletes or athletes and their coaches. Consistent messaging on mouthguard use is therefore a key injury prevention message to support athlete welfare and health and can reduce the risk of athletes needing complex or sustained restorative dental treatment.
The availability and cost of custom-made mouthguards varies globally across public, private and insurance-based healthcare systems. Public health policies that promote funding and replacement of mouthguards in sporting populations, in particular for adolescent athletes, would help to promote equity and safety. National strategies to implement mouthguard use by rule (e.g., by New Zealand Rugby Union) have been shown to reduce the risk of OFT, address psychological barriers, and normalise mouthguard use.11
More high-quality studies are needed to fully understand the greater protection of custom-made versus boil and bite mouthguards. Current recommendations are based on cohort studies, private dental insurance data, and retrospective self-reported injury studies.1,2,5,6,11 Despite this limitation, the greater comfort and stability of custom-made mouthguards are likely to influence adherence to their use.
Specific considerations for the adolescent and youth athlete
Changes in the number and position of teeth from growth and orthodontic treatment will complicate mouthguard fabrication in adolescent and youth athletes, and mouthguards will likely need to be replaced more frequently. Fabrication techniques, such as blocking out teeth that are likely to be lost as part of growth in the near future, should allow mouthguards to last for more than one season. Mouthguards can also be fabricated for children undergoing orthodontic treatment.
Mouthguard care and maintenance advice
Mouthguards should be checked as part of routine dental visits, with advice on whether they need replacement. Early adoption and encouragement of mouthguard use from grassroots and age group sports can help to normalise lifelong mouthguard use.4,12
4-step check list for mouthguard maintenance
1 – Store it: Check that the mouthguard has been kept in a clean container.
2 – Check it: Visually inspect the mouthguard to see that it is in good condition, not worn through or with any defects.
3 – Wear it: Ask the athlete to place the mouthguard in their mouth and then open wide. Make sure that the mouthguard stays in place when the mouth is open and does not need additional support to stay in place.
4 – Clean it: At the end of the session, clean the mouthguard, dry and store it in a vented container.
Mouthguards should be cleaned with a toothbrush and toothpaste or soap, followed by rinsing immediately with cool water.12 It is important to avoid exposing the mouthguard to sunlight, heat or petroleum-based products that can degrade the materials and impact the protective properties of the mouthguard.12
Summary
The use of a well-fitting mouthguard is crucial for preventing orofacial injuries in athlete competing in at-risk sports. Advice on mouthguard use should be included in routine medical guidance and education with consistent messaging on suitable fit, comfort of well-made mouthguards, lack of negative effect on performance, regular maintenance, and timely replacement of mouthguards to protect athletes. Custom-made mouthguards offer higher protection, but all athletes at risk should use a mouthguard during training and competition. Ongoing research and education are essential to further improve protective measures and athlete welfare.
Download the infographic below
Authors
Dr Irfan Ahmed1, Dr Julie Gallagher2, Professor Ian Needleman2, Ms Rachel Bower3,4, Professor Paul Ashley2, Gofrane Abdellaoui5, Dr John Haughey2, Dr Asma Aloui6, Dr Peter Fine2
1. Addenbrookes Hospital
2. UCL Eastman Dental Institute, Centre for Oral Health and Performance
3. Head Coach Rathbone Amateur Boxing Club
4. England Boxing Talent Pathway Coach
5. Muay Thai African Champion
6. High Institute of Sport and Physical Education, University of Sfax, Tunisia
Competing interests: Nil
Conceptualization: I.A., J.G., I.N., R.B., P.A. and P.F.; Data curation: A.A. and P.F.; Writing – original draft: I.A., J.G., I.N., P.A. and P.F.; Writing – review & editing: I.A., J.G., I.N., R.B., P.A., A.D., A.A. and P.F.;
Guarantor: Dr Irfan Ahmed
Acknowledgements
Patient and participant involvement (PPI)
This document was developed with the guidance of:
Rachel Bower (Current Coach and former National Amateur Boxing Champion)
Gofrane Abdellaoui (African Muay Thai Champion)
Funding, grant/award info, name and numbers: Nil
Ethical approval information, institution and number(s): N/A
References
1 – Knapik JJ, Hoedebecke BL, Rogers GG, Sharp MA, Marshall SW. Effectiveness of Mouthguards for the Prevention of Orofacial Injuries and Concussions in Sports: Systematic Review and Meta-Analysis, Sports Med 2019 Aug; 49(8):1217-1232. doi: 10.1007/s40279-019-01121-w. PMID: 31148073.
2 – Knapik J, Marshall S, Lee R, Darakjy S, Jones S, Mitchener T, Delacruz G, Jones B, Mouth guards in Sport Activities: History Physical Properties and Injury Prevention Effectiveness 2007; Sports Med 2007; 37(2) 117-144
3 – ADA Council on Access, Prevention and Interprofessional Relations; ADA Council on Scientific Affairs. Using mouthguards to reduce the incidence and severity of sports-related oral injuries. J Am Dent Assoc. 2006 Dec;137(12):1712-20; quiz 1731. doi: 10.14219/jada.archive. 2006.0118. PMID: 17138717.
4 – Ahmed I, Fine P ‘Injury prevention versus performance’: has the time come to mandate the use of mouthguards in all contact sports? BMJ Open Sport & Exercise Medicine 2021; 7: e000828. doi: 10.1136/bmjsem-2020-000828
5 – Dursun E, Ilarslan YD, Ozgul O, et al. Prevalence of dental trauma and mouthguard awareness among weekend warrior soccer players. J Oral Sci 2015;57:191-4. doi: 10.2334/josnusd.57.191
6 – Fernandes LM, Neto JCL, Lima TFR, et al. The use of mouthguards and prevalence of dento-alveolar trauma among athletes: A systematic review and meta-analysis. Dent Traumatol 2019;35:54-72. doi: 10.1111/edt.12441
7 – Fine PD, Louca C, Leung A. Sports dentistry: Principles and practice. Hoboken, NJ: Wiley Blackwell 2019:103-119.
8 – Patrick D, van Noort R, Found M. Scale of protection and the various types of sports mouthguard. Br J Sports Med 2005;39:278-81. doi: 10.1136/bjsm.2004.012658
9 – Caneppele TMF, Borges AB, Pereira DM, et al. Mouthguard use and cardiopulmonary capacity – a systematic review and meta-analysis. Sports Med Int Open 2017;1:E172–82. doi: 10.1055/s-0043-117599
10 – Ahmed I, Gordon D, Pinto JM, et al. Investigating the impact of custom-made mouthguards on maximal aerobic performance in amateur boxers .Medicine and Science in Sports and Exercise 2021; 53(8S):389-389 DOI: 10.1249/01.mss.0000763768.53311.80
11 – Quarrie KL, Gianotti SM, Chalmers DJ, et al. An evaluation of mouthguard requirements and dental injuries in New Zealand rugby union. Br J Sports Med 2005;39:650-1. doi: 10.1136/bjsm.2004.016022. Erratum in: Br J Sports Med 2006;40:186.
12 – Guidelines for the fabrication, use and maintenance of Sports Mouthguards. Available at: https://ada.org.au/getmedia/595ad4e4-9889-4e66-9be6-d433140f4d71/ADA_Guidelines_Mouthguard-Fabrication.pdf (Accessed: 04 July 2024).
Appendix
Table 1
List of “at risk” contact sports (this list is not exhaustive)
Contact sports:
Basketball, Boxing, American Football, Handball, Hockey (Ice and Field), Lacrosse, Martial Arts, Rugby, Water Polo, Wrestling, Australian Rules Football, Gaelic Football.
Limited Contact Sports and Recreational Activities:
Acrobatics, Baseball, Bicycling, Equestrian Events, Field Events, Gymnastics, In-Line Skating, Racquetball, Shot-Putting, Skateboarding, Skiing, Skydiving, Softball, Squash, Surfing, Volleyball, Weightlifting, Extreme Sports.
Table 2
| Mouthguard Type | |
| Custom made Offer the best level of protection against oro-facial and dental trauma. 6 |
Custom-made mouthguards that fit well offer the best level of protection against orofacial and dental trauma and are most comfortable to wear. Comfort is important to promote adherence to mouthguard use.4 They should be fabricated only after a full mouth/dental health assessment, and any outstanding dental treatment is completed.3 The custom-made mouthguard is constructed using an accurate impression or scan of the sportsperson’s dentition and surrounding oral structures taken by a dental professional. It ensures maximum protection, comfort, optimal uniform thickness, retention, and minimises breathing and gagging problems.12 It can be tailor-made to the individual’s request and sport.3,12 Optimal maxillomandibular occlusal relations (upper and lower teeth contacts) are also obtained. A dental professional can allow space within a custom-fitted mouthguard for development of the dentition in the young sportsperson. |
| Off the Shelf Mouthguard Types | |
| Boil & bite |
Boil and Bite mouthguards are self-moulded by impression from the athlete, after immersion in hot water.3,7,12 The fit and quality is compromised as it is dependent on the materials used and the user’s technique when forming the mouthguard. |
| Stock Mouthguards |
Stock mouthguards are prefabricated and are not moulded to fit the athlete. Stock mouthguards are liable to poor fit12 and offer the least protection against orofacial trauma. The lack of accurate fit can lead to soft tissue injuries. |